
Screening for Substance Use Disorder in Pregnancy

This article was written by Dr. Sarah Turner for the Fort Wayne Medicine Quarterly.
The opioid epidemic.
We’ve all heard this term, and we’re all aware of this issue, but I feel like many have missed that the “opioid epidemic” is being overshadowed by a Fentanyl epidemic instead. “But wait,” I hear people say – “Fentanyl IS an opioid!” True, true…it is a synthetic opioid, but put a pin in this because we are going to come back to it in just a minute. In the meantime, I’d like to talk about the population with which I specialize in working with in this terrifying new world – pregnant women and new mothers.
I remember when I was accepted into my Obstetric Fellowship, I learned that the bulk of our clinics involved working with women with substance use disorder (SUD). Pregnant women using methamphetamines, cocaine, heroin, and other illicit drugs. I was terrified at the fact that I knew absolutely nothing about this demographic and how to help them. I struggled to understand how I (a naïve young doctor who grew up on a farm in rural Canada) would be able to connect with these women. To have them trust me, and talk to me. What did we have in common that I could use to bridge a relationship with them? What was it like managing pregnant women in withdrawal? And how would I do when managing newborns in withdrawal from these substances? This unknown was really scary to me.
But this unknown became a part of medicine I fell in love with, and that I feel passionate to teach others about. SUD is not a moral failing; it is a medical disease. This is a fact that many have yet to acknowledge. Though there’s obviously more stigma associated with SUD compared to diseases like hypertension and diabetes, it is similarly caused by a combination of genetic, behavioral, environmental, and biological factors. As a society, if we ever hope to control this epidemic, we need to accept this fact. Just as we don’t shame patients with hypertension or diabetes, we should never shame patients with SUD. And just like hypertension and diabetes, we need to be screening for this disease on a very regular basis.
Pregnancy is often a period of recovery for women suffering from SUD; reproductive-age women are the most at-risk population for developing SUD. If we can identify who needs help, and assist them in taking the steps to be stable in treatment early on, not only can we decrease the risks associated with their pregnancy, but we can improve overall outcomes and long-term success rates for women. Pregnancies complicated by SUD are associated with less consistent prenatal care, and more issues with transportation, housing, and nutrition. They have increased complications, like growth restriction, preterm labor, and stillbirth. The newborns have increased risk for SIDS. These women are more likely to be victims of domestic violence and sexual abuse. Many suffer from concurrent mental illness like depression or anxiety. They have increased rates of HIV and hepatitis C. And because there’s often an obvious fear of getting in trouble, many of them have chronic medical conditions that are not being appropriately monitored or treated. When looking at how deeply SUD can affect their lives (and our community), it would seem that a simple screen would be something EVERYONE is doing, and doing well!
But it’s not.
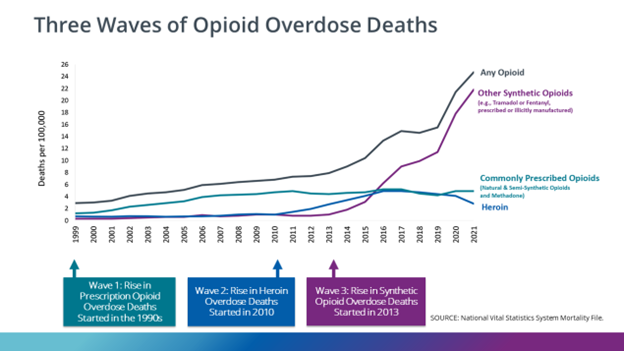
We come back to the fear of the unknown: most physicians (including many providing prenatal care) are not experienced or familiar with this area of medicine, and there’s an element of “what do I do with the positive screens?” Or if they DO know what they’re supposed to do, they may not be familiar with the local resources. When a patient tells them they’re taking Fentanyl, where do they send them? Who do they call? How can they help? For many, it’s just easier not to ask the questions, and so instead they send urine drug tests (or just not screen). It’s important that we implement universal screening, because deciding who to screen based on appearance or background will also underestimate numbers, and we will easily miss a large portion of women. There have been multiple studies looking at screening methods, and they pretty consistently show that we need to go beyond the “do you use” questions, and we shouldn’t just be sending out urine as THE screen. Using a standardized screening tool with all women has been shown to be most effective way to screen. Urine screens can grossly underestimate use, especially today. Remember that earlier point about Fentanyl being an opioid – we have only JUST gotten the ability to test for fentanyl on-site (without send-out labs that take days to weeks), but these are expensive and not readily available tests. So in reality, most urine drug screens aren’t even looking for the ONE major opioid that most people are using. Almost everything my patients are using right now is Fentanyl – the “heroin”, “Percocet”, and “Norco” are almost all actually Fentanyl pressed into the right shape, or put into the right baggy. The rise in Fentanyl overdose deaths in the last 10 years has been astronomical, while those from other opioids remain stable or have decreased.
So where does one start? We find them with screening.
We need to approach these women with compassion, respect, and with the knowledge of who to call and how to help them. We need to help maintain and protect their dignity as they take the hardest step of admitting they need our help. We need to create an environment of trust so they will want to answer these questions honestly and without fear that we will just report them to authorities (which, as it turns out, is actually illegal in Indiana). We need not to judge, but rather to provide the care that they and their babies need. If we can help recover the mother, refer the partner, have social work address the food, housing, and transportation issues, then maybe we might start building the necessary framework to have a stable home in time for baby to be born. We can empower these women to love and care for themselves the way they need and deserve to be cared for, which can not only add to the local pool of peer recovery partnerships, but can help them grow into successful members of our community. When we effectively screen, we have the potential to change lives, plural. To keep families together, or bring families BACK together. To break the generational cycle that so many of these women grew up in.
And if we approach this battle with this knowledge in knowing that a basic screen can open the door for true life change, it’s easy to see that it is probably the greatest tool we have to effectively fight this epidemic.
Be sure to join us and Dr. Tuner at our Infant and Mortality Conference on Friday, February 23rd! Register here: healthiermomsandbabies.org/conference
This article can be found in the Fort Wayne Medicine Quarterly: https://www.fwms.org/fortwaynemedicinequarterly
References
American College of Obstetrics and Gynecology. Patient Safety Bundle; Obstetric Care for Women with Opiate Use Disorder. Council on Patient Safety in Women’s Health Care. August 2017.
American College of Obstetrics and Gynecology. Opioid Use and Opioid Use Disorder in Pregnancy. ACOG Committee Opinion Number 711, August 2017 (Reaffirmed October 2021).
Substance Abuse and Mental Health Services Administration. Clinical Guidance for Treating Pregnant and Parenting Women With Opioid Use Disorder and Their Infants. HHS Publication No. (SMA) 18-5054. Rockville, MD: Substance Abuse and Mental Health Services Administration, 2018.
Substance Abuse and Mental Health Services Administration. A Collaborative Approach to the Treatment of Pregnant Women with Opioid Use Disorders. HHS Publication No. (SMA) 16- 4978. Rockville, MD: Substance Abuse and Mental Health Services Administration, 2016.
https://www.cdc.gov/drugoverdose/index.html